


Tests & Procedures
 Abdominal Ultrasound Examination
Abdominal Ultrasound Examination
Arterial (ALE/AUE) Examination
Cardiac Catheterization
Cardiac Holter and Event Monitoring
Carotid Ultrasound Examination
Computed Tomography (CT)
Echocardiography (Echo)
EKG (electrocardiogram)
MitraClip®
MUGA (Gated Pool Study)
Nuclear Stress
PET
Renal Artery Ultrasound
Stress Echocardiography
Transcatheter Aortic Valve Replacement (TAVR)
Transesophageal Echocardiography (TEE)
Vascular Testing
WATCHMAN: A One-Time Implant that Helps Reduce AFib Stroke Risk
DIAGNOSTIC SERVICES
Abdominal Ultrasound Examination
To prepare for the test, do not eat or drink anything past midnight the evening prior to your appointment. Medication may be taken with a small amount of water. This is a painless procedure. Ultrasound’s high frequency sound waves can neither harm you nor be felt. There are no known hazards associated with ultrasound procedures.
Your test will be reviewed and the results will be sent to your physician who will discuss the results with you at your next appointment.
Arterial (ALE/AUE) Examination
The arterial examination is a study to evaluate your arteries. By using high frequency sound waves to image the blood vessels, this test detects if any blockage exist within your arteries that might restrict blood flow. The test helps to determine the extent of the blockage and its location. Cuffs, similar to the ones used to determine blood pressure, will be placed on your arms and legs.
To prepare for the test, you will be asked to put on a patient gown. Wear tennis or walking shoes as you may be asked to walk on a treadmill for up to 5 minutes as part of your test. You will be asked to lie on your back so pressures can be taken of the artery. A gel applied during the procedure can be washed off with water. The test takes approximately 60 minutes.
Your test will be reviewed and the results sent to your physician who will then discuss them with you at your next appointment. If an abnormality is detected that requires immediate follow-up, your physician will be contacted immediately.
Cardiac Catheterization
Chattanooga Heart procedure brochure
Cardiac Holter and Event Monitoring
Both of these tests use machines to monitor the rhythm of electrical currents that move from one part of the heart to another. Sensors are placed on your arms, legs and chest and are connected to an instrument that records the pattern of activity with a special tape recorder. Holter monitoring requires you to wear the equipment for 24 to 48 hours and record a diary of activity. Event monitoring requires you to wear the equipment for 30 days. You have the ability to send information from event monitoring equipment to the hospital using a telephone receiver if severe symptoms occur.
Carotid Ultrasound Examination
A carotid ultrasound uses high-frequency sound waves to make pictures of your carotid arteries. The sound waves will be directed to your carotid arteries from a small, hand-held transmitter. These signals can be analyzed so that the speed of the blood flowing through your carotid arteries can be measured. The test allows us to tell your physician if there are any blockages that would interrupt blood flow from your heart to your brain. This test will also reveal any plaque along the vessels that could cause a stroke.
You will not feel the sound waves nor will they cause you discomfort. You will be asked to lie flat on your back so that pictures can be made of the carotid arteries. The test is performed on the neck region and should take approximately 50 minutes. There are no known hazards associated with the ultrasound procedure.
There is no preparation for this test and no reason to discontinue food or medications. You should wear an open neck top as the technologist will examine you from just below your shoulders to the top of your neck, at ear level.
Your carotid ultrasound test will be reviewed and the results sent to your physician who will discuss the results with you at your next appointment.
Computed Tomography (CT)
 Commonly called a CT scan or a CAT scan, this non-invasive procedure allows doctors to study cross-sections of soft tissues and organs. Our CT scanner uses cutting-edge technology to produce color, three-dimensional images of incredible clarity. Doctors use this detailed picture of your heart, veins, blood vessels and other organs to identify conditions such as coronary artery disease. The scan itself takes only about 30 seconds during which time the CT machine will take hundreds of images.
Commonly called a CT scan or a CAT scan, this non-invasive procedure allows doctors to study cross-sections of soft tissues and organs. Our CT scanner uses cutting-edge technology to produce color, three-dimensional images of incredible clarity. Doctors use this detailed picture of your heart, veins, blood vessels and other organs to identify conditions such as coronary artery disease. The scan itself takes only about 30 seconds during which time the CT machine will take hundreds of images.
Echocardiography (Echo)
This procedure uses sound waves to take “moving pictures” of the heart. These images allow doctors to see your heart in motion. This test is painless and effective in establishing specific diagnoses and estimating the severity of cardiac diseases.
EKG (electrocardiogram)
An EKG is a non-invasive test that measures the electrical signals that control the rhythm of your heart. During an electrocardiogram you will rest on a bed or chair. Small metal discs called electrodes are attached to the skin on the chest and sometimes the arms and legs. Sometimes the areas where the electrodes are placed will need to be shaved by the technician to provide a clean, smooth surface on which to attach the electrodes. The electrodes are connected to a machine that translates the electrical activity onto paper. This report is then reviewed by a physician.
 The heart is a muscular pump made up of four chambers. The two upper chambers are called atria, and the two lower chambers are called ventricles. An electrical system that occurs naturally causes the heart muscle to contract and pump blood through the heart to the lungs and the rest of the body. An EKG may show evidence of heart enlargement, signs of insufficient blood flow to the heart, heart rhythm problems, and changes in the electrical activity of the heart caused by an electrolyte imbalance.
The heart is a muscular pump made up of four chambers. The two upper chambers are called atria, and the two lower chambers are called ventricles. An electrical system that occurs naturally causes the heart muscle to contract and pump blood through the heart to the lungs and the rest of the body. An EKG may show evidence of heart enlargement, signs of insufficient blood flow to the heart, heart rhythm problems, and changes in the electrical activity of the heart caused by an electrolyte imbalance.
Tell your health professional if you are taking any medications as certain medications can affect the results of the EKG. Remove all jewelry from your neck, arms and wrists. You will need to unbutton and possibly remove your clothing above the waist. If needed, you will be given a cloth or paper covering to use during the test. For best results, lie very still during the test and breathe normally. An EKG usually takes 5 to 15 minutes to complete. There is no risk associated with an EKG.
MITRACLIP® – Advanced, minimally invasive treatment for mitral regurgitation
CHI Memorial and The Chattanooga Heart Institute are the first in the Chattanooga region to offer MitraClip® – a breakthrough technology for people who suffer from mitral valve regurgitation but are too high risk for surgical valve repair or replacement. MitraClip® therapy is the world’s first transcatheter mitral valve repair – meaning no surgical incisions are needed to deliver this lifesaving therapy.
What is Mitral Regurgitation?
Mitral regurgitation occurs when the heart’s mitral valve leaflets don’t close tightly. Heart valves work like one-way gates, allowing blood to flow in one direction between the chambers of the heart and then on to fueling your brain and other parts of your body. When these gates don’t close properly, blood can flow backwards (or regurgitate) making the heart work harder to push blood through the body. This cause shortness of breath, feelings of fatigue and worsening heart failure because of the extra strain on the heart.
People with mitral regurgitation may not realize they have the condition, because it’s often mild and progresses slowly. It’s often suspected when your doctor hears a heart murmur. Elderly people may also not realize they’re suffering from the condition since they attribute their feelings of breathlessness and general decline to old age or other health issues.
When left untreated, mitral regurgitation continues to worsen – leading to complications including atrial fibrillation, heart failure and pulmonary hypertension or high blood pressure in the arteries leading to the heart and lungs.
Identifying the Symptoms
The symptoms of mitral regurgitation are progressive, meaning they will worsen gradually as the heart works overtime to pump blood through the body. The signs and symptoms of mitral regurgitation can include:
- Blood flowing forcefully through your heart, called a heart murmur
- Shortness of breath or breathlessness when you lie down or especially with physical activity
- Fatigue or extreme tiredness, especially during increased activity
- Heart palpitations, or a sensation of a rapid, fluttering heart beat (also known as atrial fibrilaiton)
- Swollen feet or ankles
- Coughing, especially when lying down
- Excessive urination
Lifesaving Treatment – Without Open Heart Surgery
CHI Memorial is the leading provider of cardiac care, and our physicians exceed national standards for education, training and skill. That’s why we’re the first to offer this exclusive treatment for mitral regurgitation – we’re always working to provide a higher level of care for you.
Treatment for mitral regurgitation depends on the severity of your condition and if your symptoms are getting worse. If your doctor determines that open heart surgery isn’t an option for you – because of your age, advanced heart failure or other serious medical conditions – you may be eligible for the minimally invasive transcatheter mitral valve repair called MitraClip®. MitraClip® can improve your heart’s function, minimize symptoms, and help you enjoy a longer and higher quality of life.
The MitraClip® device is a small clip about the size of a dime that’s attached to your mitral valve to stop the backward leaking of blood. It treats mitral regurgitation by letting your mitral valve close more completely, helping to reestablish normal blood flow.
The CHI Memorial MitraClip® team accesses the mitral valve using a thin, flexible tube called a catheter. After the catheter is in place, the clip is guided through a vein in the leg to reach your heart. The MitraClip® is positioned over the leaky valve until it’s in the desired position. The arms of the clip are extended, and it’s passed down below the mitral valve before being pulled back up again into place. The clip grasps the mitral leaflets and then is closed. The doctors use advanced imaging systems to ensure there’s a reduction in your mitral regurgitation, and then the delivery system is removed.
Unlike surgery, MitraClip® doesn’t require opening the chest or stopping your heart. Most people who receive MitraClip® spend one night in the hospital and are released to home the next day. Although you may feel better immediately after the procedure, doctors recommend taking it easy for five to seven days to allow the site where the catheter was inserted to heal properly.
Improvements You Can Feel and See
Clinical data has shown that people who receive the MitraClip® see an immediate reduction in their mitral regurgitation – resulting in reduced hospitalizations and overall improvement in congestive heart failure – in addition to experiencing a lessening of symptoms soon after the procedure. Many patients report an immediate improvement in their shortness of breath and feelings of fatigue, leading to a much higher quality of life. It’s important to talk with your doctor about what to expect following the procedure.
Is MitraClip® Right for Me?
If you or someone you love has been diagnosed with severe mitral valve regurgitation and are not a candidate for open heart surgery, MitraClip® may be an appropriate therapy. MitraClip® is FDA approved only for patients who are considered too sick for surgery. CHI Memorial’s MitraClip® team – including cardiothoracic surgeons, imaging cardiologists, interventional cardiologists and nurse navigators – work together to determine what treatment is right for you based on your current health condition and the presence of one or more surgical risk factors.
For more information or to schedule an appointment for an evaluation, please call CHI Memorial’s MitraClip® Valve Coordinator at (423) 495-4327.
MUGA (Gated Pool Study)
A MUGA examination allows your physician to calculate how well your heart is beating. This can then be used to determine the condition of the heart muscle and its response to any medication that is given.
When you arrive at our nuclear department, you will be given an injection of a medicine that will need to circulate in your body for 30 minutes. After this time, an IV will be started. You will be placed on a table under a camera and injected with a minute amount of radioactive material that will allow us to obtain images of your heart beating. (The radioactive tracer gives minimal exposure and is eliminated from the body in approximately 24 hours.)
The imaging process will take approximately 30 minutes. The entire study takes about 90 minutes.
Continue to take your scheduled medications if you are pregnant, or may be pregnant, or if you are nursing, tell your physician and technologist prior to the study. It is best for women of childbearing age to have the examination done during the first 10 days following the onset of the menstrual cycle.
Nuclear Stress
The heart receives its blood from blood vessels called coronary arteries. If these arteries become partially blocked or narrowed by atherosclerotic heart disease or hardening of the arteries, the heart may not receive the blood it needs. At rest, the heart uses less blood than when it is working. This test exercises your heart to determine if there is any decrease in blood flow to one area of the heart and how much heart muscle is involved.
An IV will be started and you will be injected with a radiopharmaceutical. After 30-45 minutes, you will lie on an exam table for approximately 20 minutes for a scan of your heart.
If you’re having the exercise stress test, you’ll be connected to an EKG machine and will walk on a treadmill as long as you can. You’ll then be injected with a second dose of the medication and taken to a scan room for another 20 minute scan.
If you are having the medicine stress test (which utilizes a vasodilator medication), you’ll be connected to an EKG machine while sitting down. You’ll be injected with a medication that will cause arterial (coronary vessels) vasodilation and increase coronary blood flow. You will then be given a second dose of the radiopharmaceutical medication, wait 30-60 minutes, then will have a second scan which will last 15-20 minutes. The vasodilator medication increases blood flow in normal coronary arteries with little increase in stenotic arteries (vessels with blockage). This causes a difference in myocardial perfusion intensity so that at the end of the test, the imaging physician can potentially identify the part of the heart muscle which is not getting enough blood flow due to a blockage. This test may increase heart rate and lower blood pressure, briefly cause shortness of breath, headache and flushing but all these symptoms will usually resolve within a few minutes.
The approximate time of your visit will be three hours. If you experience chest pain, or any other problems during your stress test, our medical staff is well trained to assist you and there is always a cardiologist present for your safety.
IMPORTANT: Do not eat or drink anything (except water) for at least 6 hours before your test. You may drink as much water as you wish unless you are on fluid restriction. Do not have any caffeine (coffee, chocolate, tea, etc.) for 24 hours before your test.
If you are insulin-dependent diabetic, call the Cardiac Imaging Department at (423) 697-2187 for special instructions.
Because you will exercise, you should wear comfortable footwear and comfortable clothes, preferably slacks. For this portion of the test, you will need to undress from the waist up and put on a hospital gown so that the EKG patches can be applied to your chest. We suggest you wear a light sweater or jacket as imaging room temperatures must be kept cool.
IMPORTANT INSTRUCTIONS ON YOUR MEDICATIONS:
Some medications should not be taken the day before and day of the test. Please read these instructions thoroughly to ensure your test can be performed satisfactorily.
For all patients: Nitroglycerin patches should be removed the night before the test.
Reminder: Bring your medications with you the day of the test.
Your test will be reviewed and the results sent to your physician who will discuss them with you at your next appointment. The technologist cannot give out results.
PET
Cardiac PET (Position Emission Tomography) exams help evaluate the blood supply and function of the heart. It is useful in detecting how adequate the blood supply is to the heart muscle.
How is this test performed?
After you have arrived and registered for your test, a technologist will ask you some questions about your medical history. An IV will be inserted in your hand or arm.
You’ll have tabs placed on your chest for an EKG which will monitor electrical activity of your heart throughout the study. You’ll lie down on the scanner table on your back with both arms above your head (if you’re able). You’ll be given a small amount of radiopharmaceutical through your IV that allows us to image your heart at rest. Shortly after that, you’ll be given a pharmaceutical called a vasodilator that will increase the flow of blood to the arteries of the heart, similar to the effect of exercise and your heart will be imaged a second time.
How should I prepare for the test?
Do not eat or drink anything (except water) for at least 6 hours before your test. You may drink as much water as you wish unless you are on fluid restriction. Do not have any caffeine (coffee, chocolate, tea, etc.) for 24 hours before your test.
IMPORTANT INSTRUCTIONS ON YOUR MEDICATIONS:
Some medications should not be taken the day before and day of the test. Please read these instructions thoroughly to ensure your test can be performed satisfactorily.
If you are insulin-dependent diabetic, call the Cardiac Imaging Department at (423) 697-2187 for special instructions.
We suggest you bring a jacket or sweater with you as the imaging area must be kept cool.
Renal Artery Ultrasound
This ultrasound test checks the renal arteries that lead to the kidneys for narrowing or blockages which could lead to high blood pressure. It is also used to check the arteries after surgery, angioplasty or stenting.
This is a painless procedure. Ultrasound’s high frequency sound waves can neither harm you nor be felt. There are no known hazards associated with ultrasound procedures.
The test will be performed while you are lying on your back in a bed. You may be asked to roll from one side to another. A gel is applied to your abdomen and an ultrasound probe is run along the skin following the path of the arteries.
To prepare for the test, don’t eat or drink anything past midnight the evening before your appointment. Medication may be taken with a small amount of water. Wear comfortable clothing for easy access to abdomen area.
Your test will be reviewed and the results will be sent to your physician who will then discuss the test results with you at your next appointment. The technologists cannot give you your test results.
Stress Echocardiography
 Like with a regular echocardiography, sound waves are used to examine the heart’s movement. Four standard views of the heart are taken while you are at rest, and the same four views are taken after you perform an exercise treadmill test. The purpose is to make sure the heart is getting enough blood flow and oxygen when it is under stress—such as when the heart rate is increased during an activity like walking on the treadmill. These images help doctors discover and treat blockages and other conditions before they become serious or life threatening. Medication can be used to elevate the heart rate if you are unable to use the treadmill.
Like with a regular echocardiography, sound waves are used to examine the heart’s movement. Four standard views of the heart are taken while you are at rest, and the same four views are taken after you perform an exercise treadmill test. The purpose is to make sure the heart is getting enough blood flow and oxygen when it is under stress—such as when the heart rate is increased during an activity like walking on the treadmill. These images help doctors discover and treat blockages and other conditions before they become serious or life threatening. Medication can be used to elevate the heart rate if you are unable to use the treadmill.
Transcatheter Aortic Valve Replacement (TAVR)
CHI Memorial’s Heart Valve Program offers a revolutionary procedure for the treatment of severe aortic valve stenosis (narrowing of the aortic valve opening).
Transcatheter aortic valve replacement (TAVR) is a minimally invasive procedure that enables a collapsible aortic heart valve to be placed inside the heart. During the procedure, the TAVR device is crimped down and placed into the body via a catheter that is inserted in the upper thigh or groin. Once it’s delivered to the site of the patient’s diseased valve, the device is expanded with a balloon and begins to work immediately.
TAVR offers some patients the potential of a longer, better quality life. When TAVR was first introduced, it was only approved for patients who were not candidates for traditional open-heart surgery. Changes to the requirements now mean that patients with valve disease who are deemed high or intermediate risk may also be appropriate.
To assess whether someone is a candidate for TAVR, patients with severe aortic valve disease are screened in CHI Memorial Hospital’s Heart Valve Program. This program is directed by a team of specially trained cardiovascular surgeons, interventional cardiologists, and imaging cardiologists who review possible candidates to determine if TAVR is the best course of treatment for each individual patient.
CHI Memorial is the only hospital in the Chattanooga area chosen as a site for the use of the TAVR valve. More than 325 patients have been treated with lifesaving TAVR therapy at CHI Memorial.
EVOLUTION OF TAVR
The Edwards SAPIEN Valve was the first TAVR therapy to receive FDA approval. In October 2011, when CHI Memorial was selected, it was one of only 24 hospitals nationwide chosen to use the device. CHI Memorial performed the third implant in the nation using the FDA approved SAPIEN device. A smaller retroflex valve delivery system for TAVR was approved in June 2014 and often requires no surgical incision – it can be placed through a small puncture site in the groin.
To learn more about CHI Memorial’s Heart Valve Program, talk with your physician or call the valve clinic coordinator at (423) 495-4327.
Transesophageal Echocardiography (TEE)
The transesophageal echocardiography enables doctors to view the heart through a small, flexible tube called an endoscope which is inserted through the esophagus. This probe is small enough and long enough to reach the heart and allows doctors to closely evaluate the heart and blood vessels within the chest. This test is used to assess the heart’s functions and structures and is also used during surgery to evaluate the effects of surgical intervention to the heart. For this procedure, you are sedated.
Vascular Testing
This type of testing collects information about your blood vessels and the way blood passes through them. An ultrasound is commonly used to gather real-time information about blood flow activity. Doctors are able to utilize this information, along with blood pressure measurements, to gauge arterial and venous flow. The results from these tests help physicians diagnose disorders in the blood vessels.
WATCHMAN: A One-Time Implant that Helps Reduce AFib Stroke Risk
How Does AFib Increase Stroke Risk?
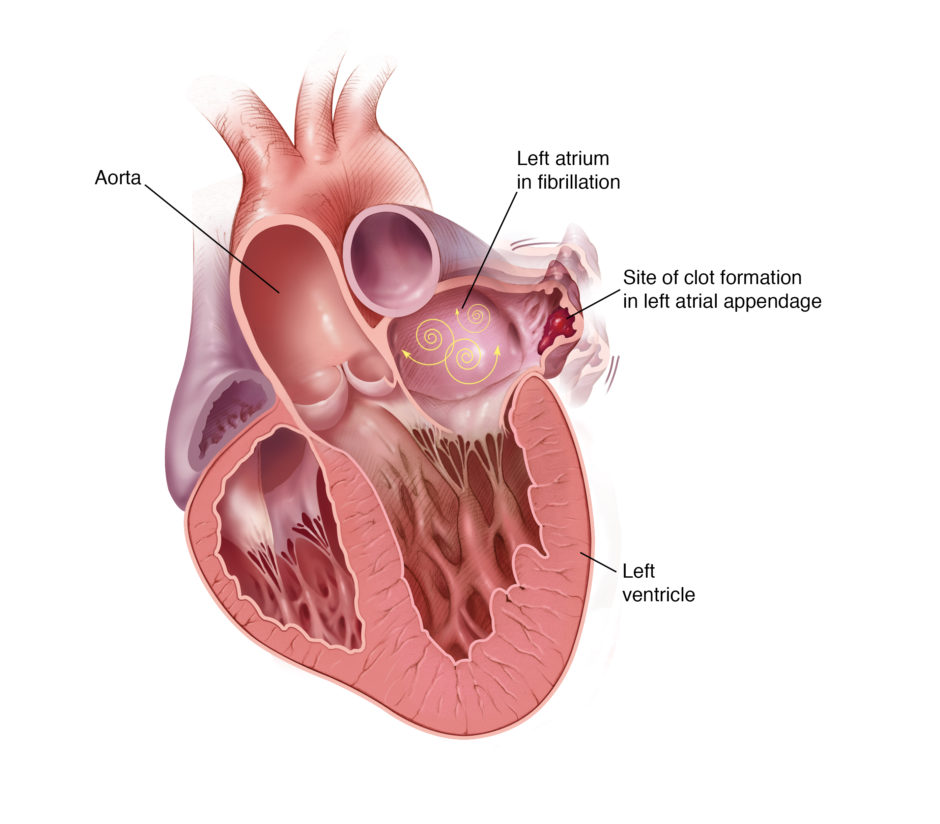
The average person with atrial fibrillation (also called AFib or AF) is five times more likely to have a stroke than someone with a regular heartbeat.1 That’s because AFib can decrease the heart’s pumping capacity by as much as 30%.2 Because blood isn’t pumped out of the heart normally, it’s easier for blood cells to stick together and form clots in an area of the heart called the left atrial appendage (LAA).2, 3 When a blood clot escapes from the LAA and travels to another part of the body, it can cut off the blood supply to the brain, causing a stroke.1, 4
Learn more about atrial fibrillation and stroke risk.
In people with atrial fibrillation not caused by heart valve problems (the most common type of AFib), more than 90% of stroke-causing clots that come from the heart are formed in the LAA.3
Learn more about types of AFib, symptoms and risks, and treatment for Afib.
Reducing AFib Stroke Risk
Blood thinners, also called anticoagulants, are an effective way to lower the risk of stroke in people with atrial fibrillation not caused by heart valve problems.5 Common blood thinners include warfarin (also known as Coumadin®), Eliquis®, Pradaxa®, Xarelto® and Savaysa®.
But some people need an alternative to blood thinners, because they can increase the risk of bleeding.5 Some bleeding events are minor and easily treated, like a cut taking longer than normal to stop bleeding. In other cases, the bleeding can be life-threatening, such as when bleeding in the brain causes a stroke.
If you have a history of bleeding or a lifestyle, occupation or condition that puts you at risk for bleeding, your doctor may consider an alternative to blood thinners, such as the WATCHMAN Implant.
An Alternative to Blood Thinners
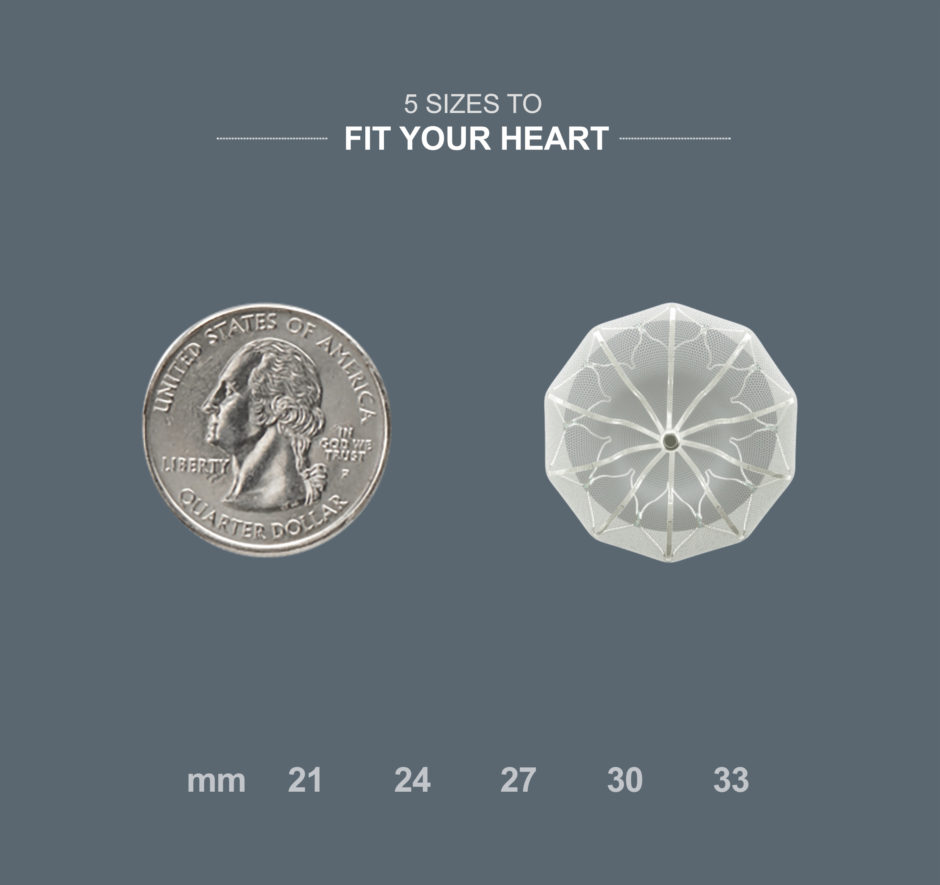
WATCHMAN is a permanent implant that offers an alternative to the lifelong use of blood thinners. It’s about the size of a quarter and made from very light and compact materials commonly used in many other medical implants.
How WATCHMAN Works
WATCHMAN effectively reduces the risk of stroke by permanently closing off the LAA to keep blood clots from escaping. WATCHMAN can eliminate the bleeding risks and regular blood tests and food-and-drink restrictions that come with warfarin. In a clinical trial, 9 out of 10 people were able to stop taking warfarin just 45 days after the WATCHMAN procedure.

How is WATCHMAN Implanted?
WATCHMAN is implanted into your heart in a one-time procedure. To implant WATCHMAN, your doctor makes a small cut in your upper leg and inserts a narrow tube, as done in a standard stent procedure. Your doctor then guides WATCHMAN into your heart’s LAA. The procedure is done under general anesthesia and takes about an hour. Patients commonly stay in the hospital overnight and leave the next day.
After the Procedure
Following the WATCHMAN procedure, you’ll take warfarin for 45 days or until your LAA is permanently closed off. During this time, heart tissue will grow over the implant to form a barrier against blood clots. Your doctor will monitor this process by taking pictures of your heart to see when you can stop taking warfarin.
Your doctor will then prescribe a medicine called clopidogrel (also known as Plavix®) and aspirin for you to take for six months. After that, you’ll continue to take aspirin on an ongoing basis. A very small number of patients may need to keep taking blood thinners long term.
In a clinical trial:
- 92% of patients were able to stop taking warfarin just 45 days after the procedure6
- 99% of patients were able to stop taking warfarin within 1 year after the procedure6
Is WATCHMAN Right for You?
If you have a history of bleeding or a lifestyle, occupation or condition that puts you at risk for bleeding, WATCHMAN may be right for you. But like any medical procedure, WATCHMAN comes with risks, so it isn’t right for everyone. Your cardiologist will weigh your risk of a stroke against your risk of a serious bleeding problem to determine the right treatment for you.
Take the WATCHMAN Assessment to see if WATCHMAN is right for you.
Hear from a WATCHMAN Patient
When atrial fibrillation and the bleeding risks of blood thinners started to slow down Ingrid, an active 55-year-old, she talked to her doctor about an alternative treatment. See how WATCHMAN helped give her a new lease on life.
Watch Ingrid’s Story
Getting WATCHMAN
The first step to finding out if you’re a candidate for WATCHMAN is making an appointment with a cardiologist to discuss your options.
For more information, call (423) 697-3550.
WATCHMAN is for people with atrial fibrillation not caused by a heart valve problem who need an alternative to warfarin. This website is intended to provide patients and caregivers with some information about the WATCHMAN Implant. It may help prepare you for talking to your doctor about your options for reducing stroke risk.
Important Safety Information
The WATCHMAN Device is a permanent implant designed to close the left atrial appendage in the heart in an effort to reduce the risk of stroke.
With all medical procedures there are risks associated with the implant procedure and the use of the device. The risks include but are not limited to accidental heart puncture, air embolism, allergic reaction, anemia, anesthesia risks, arrhythmias, AV (Arteriovenous) fistula, bleeding or throat pain from the TEE (Trans Esophageal Echo) probe, blood clot or air bubbles in the lungs or other organs, bruising at the catheter insertion site, clot formation on the WATCHMAN™ Closure Device, cranial bleed, excessive bleeding, gastrointestinal bleeding, groin puncture bleed, hypotension, infection/pneumonia, pneumothorax, pulmonary edema, pulmonary vein obstruction, renal failure, stroke, thrombosis and transient ischemic attack. In rare cases death can occur.
Be sure to talk with your doctor so that you thoroughly understand all of the risks and benefits associated with the implantation of the WATCHMAN Device.
Sources
- National Stroke Association. Making the Afib-Stroke Connection. https://www.stroke.org/sites/default/files/resources/Afib-Connection%20for%20hcp.pdf. Published 2012. Accessed September 1, 2016.
- Harvard Health Publications. Atrial fibrillation. http://www.health.harvard.edu/heart-health/atrial-fibrillation-common-serious-treatable. Harvard University Medical School. Published November 2011. Accessed August 25, 2016.
- Blackshear JL, Odell JA. Appendage obliteration to reduce stroke in cardiac surgical patients with atrial fibrillation. Ann Thorac Surg. 1996;61:755-759.
- Cleveland Clinic. Atrial fibrillation (Afib). http://my.clevelandclinic.org/services/heart/disorders/arrhythmia/atrial-fibrillation-afib. Published May 2015. Accessed August 25, 2016.
- National Stroke Association. Making the Afib-Stroke Connection. https://www.stroke.org/sites/default/files/resources/Afib-Connection%20for%20hcp.pdf. Published 2012. Accessed September 1, 2016.
- Holmes DR Jr, Kar S, Price MJ, et al. Prospective randomized evaluation of the Watchman Left Atrial Appendage Closure device in patients with atrial fibrillation versus long-term warfarin therapy: the PREVAIL trial. J Am Coll Cardiol. 2014;64(1):1-12.